The Macmillan End-of-Life Care Fund
Tags

For too many people, the last months of life involve frequent hospital admissions, fragmented care, and missed opportunities to be supported at home.
The Macmillan End-of-Life Care Fund – a £36 million investment by Macmillan Cancer Support developed in partnership with Social Finance – was designed to shift the dial on palliative and end-of-life care by supporting the NHS and local providers to deliver innovative services in the community for people at end of life.
This Fund also provided evidence to support the development of the Neighbourhood Transformation Fund model, launched in 2025.

Most people at end of life don’t want to spend more time in hospital than is absolutely necessary. Almost always they’re going to be more comfortable and less anxious in their own environment.
Mary Walding, Lead Specialist Nurse for Palliative Care, Oxford University Hospitals Foundation NHS Trust (OUH)
How the Macmillan-End-of-Life Care Fund works
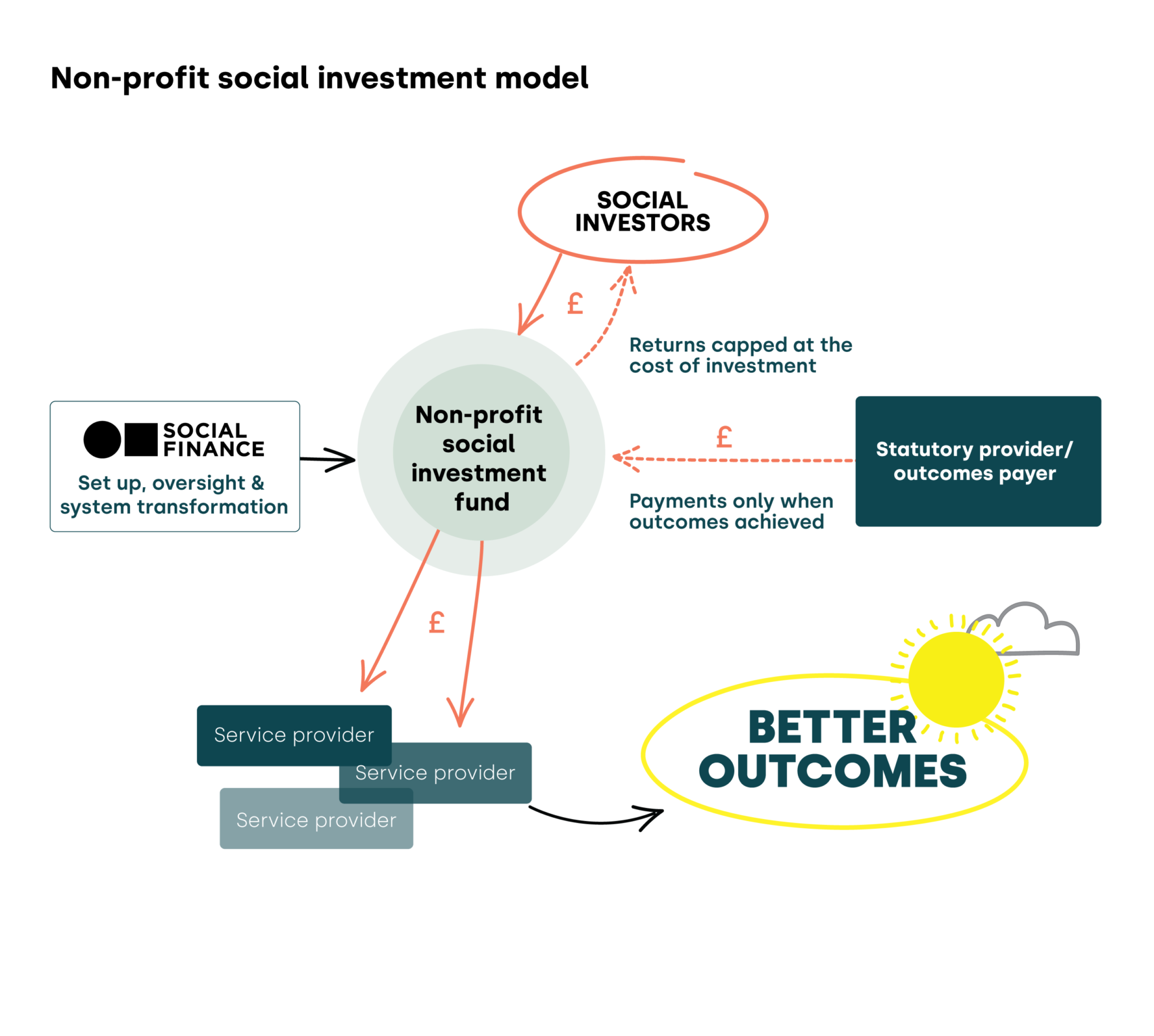
The Fund uses a pioneering ‘non-profit’ model of social investment, where the investor (in this case Macmillan) does not receive a return on investment, and outcomes payments are capped at the cost of delivering the service.
The upfront funding and wrap-around support provided by Social Finance and in this case by the social investor Macmillan, gives NHS teams and local providers the head space and skills they need to design and deliver innovative services.
By working in partnership, we help ensure people in their final year of life receive the right care, in the right place, at the right time – whilst also easing pressure on NHS hospitals so others can get the treatment they need.
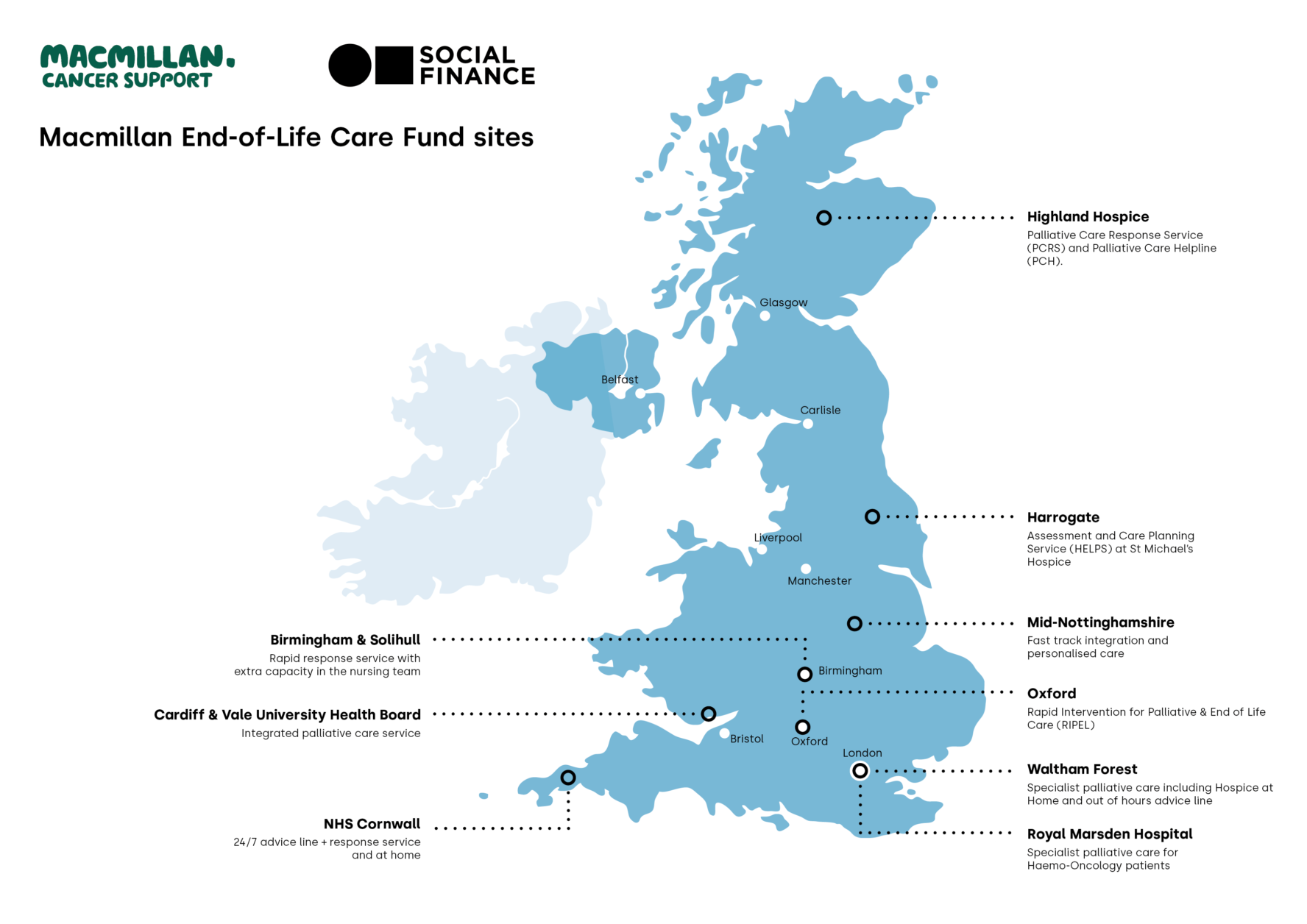
Where the Macmillan EOLC Fund has invested
The Macmillan End-of-Life Care Fund has invested into nine sites across the UK.
The first of these to launch – the Rapid Integrated Palliative and End-of-Life (RIPEL) in Oxford – was instrumental in helping us build the case for the Neighbourhood Transformation Fund.
Oxford’s Rapid Integrated Palliative and End-of-Life (RIPEL) services
The Rapid Integrated Palliative and End-of-Life (RIPEL) in Oxford was the first project launched through the Macmillan End-of-Life Care Fund and is a strong exemplar of how the Fund works in practice.
RIPEL was created to address a significant gap in community-based care for people nearing the end of life in Oxfordshire and South Northamptonshire. Before RIPEL, people in their final 90 days were being admitted to hospital on multiple occasions because there wasn’t enough support in the community.
In 2022, in a unique partnership between Macmillan, Social Finance, Oxford University Hospitals Foundation NHS Trust (OUH) and the Sobell House Hospice Charity, four connected RIPEL services were mobilised in Oxford. The aim was to reduce emergency admissions for people at the end of life and to improve provision of community-based care:
- Palliative Care Hub: A rapid-response phone service run by a team of specialists who coordinate care across different parts of the system.
- Hospice Outreach: A “virtual ward” that allows people to receive safe, high-quality care at home instead of being admitted to hospital.
- Home Hospice: Helps people who wish to spend their final days at home, providing the care and support they need there.
- Hospital Rapid Response: Supports patients to leave hospital sooner if they are approaching the end of life and prefer to be cared for elsewhere.
Evidence of impact
Over the three years of the programme, RIPEL made a clear and measurable difference. People using these services spent significantly fewer days in hospital during the last weeks of life. This meant hospital beds and staff time could be reallocated to patients who needed active treatment.
The success of RIPEL not only in improving outcomes for patients and their families, but also in freeing up hospital resources, means that the outcomes-payer, OUH, has continued to fund the services after the social investment period ended in 2025.
Benefits of using the Macmillan End-of-Life Care Fund
- Up-front funding to get the innovative service off the ground without the NHS Trust or Integrated Care Board being exposed to financial risk.
- Expert support from Macmillan and Social Finance to help define the problem, to identify gaps in existing provision and to understand what kind of service might address those needs.
- Expertise in partnership working that includes negotiating and setting up outcomes contracts between all relevant parties.
- NHS staff have the time and headspace they need to collaborate with colleagues across the health and care system, to design a new service that’s tailored to local requirements.
- Wrap-around training and technical support for service providers to help them gather and analyse data needed for performance management, and to trigger outcomes payments.

Not only did we get up-front funding, we also had access to the expertise and experience of the teams at Social Finance and Macmillan. They helped us define what it was that we were trying to achieve… and to ask, how can we make this sustainable? How can we demonstrate that it’s actually value for money? It also allowed us to be brave, knowing we had time to test it out and redesign.
Professor Bee Wee CBE, Consultant in Palliative Medicine and Medical Director of the Rapid Integrated Palliative and End-of-Life (RIPEL) services, OUH

If a patient phones into the Palliative Care Hub they will get prioritised, they will get spoken to that day. A plan of action will come out of that. If they are unstable, they will be seen [in the community]. And that’s just something that didn’t happen before RIPEL.
Mary Walding, Lead Specialist Nurse for Palliative Care, RIPEL

One of the most telling outcomes for me is when I see how proud our staff are of the service and knowing that our staff can actually do their job better than they could before. Now rather than telling a patient that they’re just going to have to go to the Emergency Department to get the level of care they need – we can support them at home.
Kerri Packwood, RIPEL Programme Manager, OUH
Why did we focus on end-of-life care?
In 2015 Social Finance launched the Care and Wellbeing Fund to test different models of social investment in health and social care. Macmillan Cancer Support and Big (now Better) Society Capital each invested £6 million into this Fund.
Over 10 years of the Fund, seven end-of life care focussed Social Outcomes Contracts were invested into, giving each service up-front funding and expert wrap-around support from Social Finance.
Two services in particular – the Your Life Line 24 Hour Service in Hillingdon, North London and the Marie Curie Responsive Emergency Assessment and Community Team (REACT) in Bradford – demonstrated the benefits of using a Social Outcome Contract model in palliative and end-of-life care.
By mobilising innovative community-based services tailored to meet local needs, not only were outcomes improved for people in the last year of life, but NHS resources (hospital bed days) could be re-allocated to those needing acute services and treatment.
All of us would like to die a ‘good’ death, and for the majority of us that means not being in hospital.
This also makes financial sense for the NHS and the public purse.
The report Public Expenditure In the Last Year of Life commissioned by Marie Curie from the Nuffield Trust and Health Economics Unit, published in February 2025, sets out some stark findings about the costs of caring for people in the last year of life.
In addition Marie Curie’s Better End of Life Report 2024 concluded “too many people are unable to access the joined-up care and support they and their unpaid carers need at the end of life. Community support for palliative care is inadequate, with GP and District Nursing services stretched beyond capacity. There are no two ways about it: care for dying people is in crisis.”
What is palliative and end-of-life care?
Palliative and end-of-life care supports people with advanced, progressive, incurable illness to live as well as possible until they die and to die a ‘good death’.
For many a ‘good death’ means being without pain, in a familiar place with friends or family and being treated with dignity and compassion.